Dr. Paulo Malo, a dentist in Portugal, in cooperation with Nobel Biocare, has developed what he calls the “All-on-Four” technique for dental implants.
 The problem he is trying to address is restoring the mouths of patients who have lost all their teeth and don’t have much bone left to retain dental implants. Often these patients require extensive bone grafting procedures, which are time-consuming and expensive.
The problem he is trying to address is restoring the mouths of patients who have lost all their teeth and don’t have much bone left to retain dental implants. Often these patients require extensive bone grafting procedures, which are time-consuming and expensive.
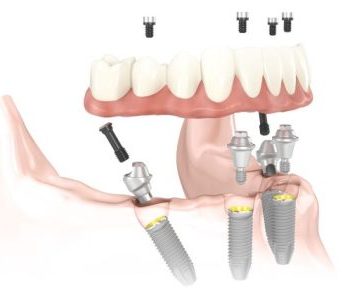
Dr. Malo found that if he placed all the implants in the anterior of the jaw, where there is usually better bone density, and if two of those implants were highly angled, as shown to the right, they could provide stable support for a complete denture.
The radiograph and diagram below illustrate this technique.
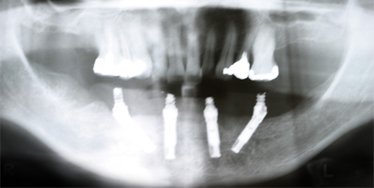
Radiograph of All-on-Four dental implants
Here is a panographic x-ray of the four angled implants that have been placed.
You can see that two of the implants are highly angled. But notice that the exposed tips of the dental implants, the part sticking out of the bone, are all pointed upward and are relatively parallel.

Placing a denture over All-on-Four dental implants
On the right you can see that when the denture is screwed on, the screws are all placed normally, because the angulation all occurs under the surface of the tissue.
But this technique isn’t without its critics. One renowned implant dentist in Phoenix who has pioneered other techniques, after thoroughly studying the All-on-4 technique, is concerned about its risks. If one of the implants fails, the entire mouth has to be re-done, and he feels that this is an unacceptable level of risk. Some leading implant dentists have been reporting higher rates of failure with this technique. Still, others feel that there is no increased risk. The technique has been gaining in popularity, and the consensus among implant dentists seems to be in favor of this technique. Some, who are worried about the risks, will add two implants and do what they call an All-on-6 technique.
We advise you, before you have your dentist use this technique for you, that you be sure your dentist is highly experienced and willing to stand behind his or her work.
Click here to ask Dr. Hall a question.
Click here for referral to an expert cosmetic dentist.
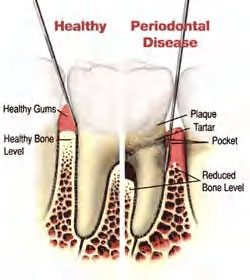 going into these pockets with instruments and cleaning out the calculus. When you have gum disease, it’s important that these pockets be cleaned out thoroughly.
going into these pockets with instruments and cleaning out the calculus. When you have gum disease, it’s important that these pockets be cleaned out thoroughly.

