Restoration of fractured teeth —a long-term study.
by David A. Hall, D.D.S.
Dr. Sergio A.M. Ourique
Dr. Guilherme H. Itikawa
(Dr. David Hall is a dentist who practiced in Cedar Rapids, Iowa, and is now the owner and president of Infinity Dental Web of Phoenix, Arizona.)
(Dr. Sergio Ourique is Chairman of the Department of Prosthodontics, University of Sao Paulo, Sao Paulo, Brazil.)
(Dr. Guilherme Itikawa is an endodontist practicing in Sao Paulo, Brazil.)
This research was published in a Brazilian dental journal, Revista Paulista de Odontologia, Jan-Feb 2004, pp. 10-15.
Click here for the Portuguese translation.
The English version of this article was published in the
Journal of the Colorado Dental Association, Fall 2004 issue.
Note: This research has been replicated by Divia, Joseph, and Varughese, at the University of Kerala, India. See their case report, “Complicated Tooth Fracture Management“, published in the IOSR Journal of Dental and Medical Sciences, July, 2015.
Abstract:
When a vertical tooth fracture extends below the gingival attachment, the recommended treatment has been extraction.[1][2][3][4][5][6]As asserted by Walton, after the diagnosis of a split tooth is confirmed, saving the tooth is not an option. “Maintaining an intact tooth is impossible,” the text explains. “If the fracture is severe (that is, deep apically), the tooth must be extracted. If the fracture shears to a root surface that is not too far apical, the smaller segment will be very mobile. Then there is a good possibility that the small segment can be removed and the remainder of the tooth salvaged.
The rationale is that when a fracture extends from the supragingival area to below the attachment, the fracture line can become a nidus for progressive inflammation. As stated by Simon, Glick and Frank, “Once this attachment is breached and the groove becomes involved, a self-sustaining infrabony pocket can be formed along its length. This condition is nonresponsive to periodontal treatment.”[7]
This paper will challenge these assertions by offering literature citations and long-term case studies of up to twenty years which show conditions under which a split or fractured tooth can be completely salvaged, intact and fully healthy.
Background:
Roots are, of course, covered with cementum. Cementum is generated from the periodontal ligament. We have known for a long time that cementum deposition occurs throughout life.[8] Theoretically, then, if there is an injury to a root such as a crack, if the proper conditions are maintained, the potential exists for that crack to be able to heal over with new cementum
There have been a few reports of such healing in the literature. Hammer[9] studied tooth fractures in dogs and noted, after two weeks, dentin repair beginning on the pulpal side of the fracture, and cementum repair on the fracture line after three weeks.
Andreasen and Hjørting-Hansen demonstrated in a study published in 1967 that cementum healing apparently occurs in humans.[10] In a study of 50 horizontal root fractures, they showed the apparent formation of new cementum, radiographically, when the fractured segments were in close apposition. One of these teeth was extracted and it showed, clinically, the formation of cementum and cementoid.
Andreasen and Hjørting-Hansen concluded that the two most important features in the successful treatment of root fractures are immediate reposition and fixation.
The above are horizontal root fractures that are entirely below the gingival attachment. Can the same processes work to heal vertical fractures that traverse the attachment?
In an earlier case report by Hall, a central incisor in an 11-year-old male that was shattered into four pieces, was restored.[11] The trauma had caused several vertical fractures which traversed the gingival attachment. Eighteen months postoperatively, in spite of pulpal involvement in the fractures, the tooth was still vital and apparently completely healthy. However, subsequent to the initial success of the treatment, the tooth was re-fractured in a second traumatic incident. Upon examining the second injury, Hall was able to separate the coronal portions of the injury very slightly, but the resistance to separation of the radicular portions was consistent with cementum healing having occurred over the first injury. Repair was attempted after the second injury, but without long-term success. Five years later, the tooth was extracted. However, the incident suggested a possibility of true cementum healing of a vertical root fracture.
In the 1980’s, Masaka[12] developed a technique for preserving teeth with vertical root fractures using a 4-META adhesive. He has extracted fractured teeth, repaired them extraorally, and replanted them. While his success validates the concept of root fracture repair, it doesn’t address the issue of potential biological cementum repair. Aouate[13] has also done work in similar vertical root fracture repair with 4-META in France.
Report of Cases:
Case #1
On September 8, 1992, the patient, a 72-year-old white male, presented with a tooth that had been very tender to biting for about ten days, and the pain had increased during the previous 24 hours. Visual examination disclosed a mesio-distal fracture through the furcation of the tooth. With no pressure on the tooth, the fracture was not noticeable, but the buccal and lingual halves of the tooth could be separated upon pressing an explorer tine into the central groove (see figures 1[14] and 2[15]). There were no restorations in the tooth. Tooth #4 was missing its lingual cusp. The patient said this cusp had broken off approximately 12 years earlier. There was also a missing disto-buccal cusp on tooth #18, with an existing small occlusal amalgam in the central pit of this tooth.
The patient’s periodontal history showed existing periodontitis with occasional pocketing of 4-6 mm. in various areas of his mouth. Probing tooth #3 revealed no pathological pocketing.
The patient’s medical history showed existing diabetes mellitus. The patient had also had a myocardial infarction in April 1989. Current medications included Procardia, aspirin, Tenormin, Diabeta and Synthroid.
A Hygienic #3 rubber dam clamp was tied with floss and placed on the tooth, holding the fractured halves of the tooth together. The segments were lined up perfectly, so that there were no cracks or spaces between them. 1.8 ml of lidocaine with 1:100,000 epinephrine was injected into the buccal alveolar mucosa.
A crown preparation was begun and a groove about 3-4 mm. deep was cut into the central groove of the tooth along the lines of the fracture (figure 3[16]). The groove was etched with 37% phosphoric acid for 10 seconds, dried, and Tenure® A&B (DenMat) were placed. That was dried, and Scotchbond II® Dual Cure (3M Dental Products) bonding resin was placed. The groove was filled with Z-100® (3M Dental Products) composite, and this was cured for 60 seconds with a halogen curing light. The crown preparation was completed and an aluminum shell temporary crown was placed, lined with acrylic and cemented with Zone® (Cadco) temporary cement
The patient was seen the following day, and the temporary crown was removed and vitality tests were performed. The tooth appeared to respond normally to cold tests. The temporary crown was re-cemented.
The patient was seen again six days later, and a vinyl polysiloxane final impression was taken using a custom tray (see figure 4[17]). He was seen again two days later complaining of pain in the tooth. A periapical radiograph disclosed widening of the periodontal ligament space near the apex of tooth #3. An opening was made through the temporary crown and into the pulp chamber, and the canals were instrumented with k-files. It was left open for four days and then filled with gutta percha cemented with a calcium hydroxide cement. A #5 titanium Parapost® (Whaledent) was placed into the lingual canal. The inside of the access opening was etched with 37% phosphoric acid, Tenure® (DenMat) was placed, and Core Paste® (DenMat) was placed into the opening.
Two days later, a permanent cast gold crown was cemented with GlasIonomer® (Shofu) crown and bridge cement.
Nine months later, the patient presented for a maintenance examination. He reported that about 3 to 5 months after the crown was placed, that the tooth started hurting and he developed a “pus bag” in the buccal area near the tooth. The pain then disappeared and had felt normal since.
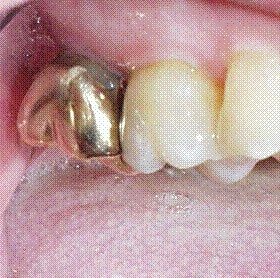
In December 1993 he presented for another examination. There was a small amount of exudate coming from the sulcus around tooth #3, but no pain. We elected to leave it alone. In June, 1994, he presented again, and the tooth was asymptomatic, with a 5 mm pocket on the mesial. We continued to check it annually and radiograph it periodically. In June 2002, almost 10 years after the mesio-distal fracture, it was again examined, radiographed, and photographed. The tooth had a normal sulcus all the way around, and no pathology was detected on the radiograph. The tooth was asymptomatic (see figures 5[18] and 6[19]).
Similar results have been seen in other tooth fracture cases.
Case#2
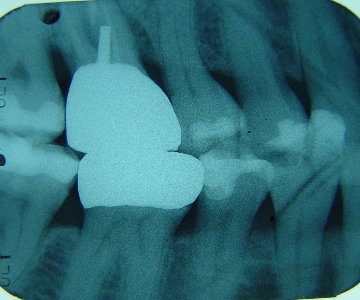
In December 1980, a patient presented with a mesio-distal fracture through the furcation of tooth #2, which had just had endodontic treatment. The tooth was clamped, filled with Tytin® amalgam (Kerr) prepared with dovetails into each half of the tooth, and then prepared for a full cast crown. There were no post-operative complications – no pain or swelling. Examination in August 2001 showed the tooth with a normal sulcus, and no pain or pathology noted (see figures 7[20] and 8[21]).
Case #3
In July 1987 a patient presented with a fractured tooth #15, which had an existing endodontic treatment and amalgam restoration. This fracture was through the furcation and continued down the palatal root. The fracture was reduced, clamped, and stabilized with Tytin® amalgam (Kerr), and a full cast crown was placed. Pain and swelling persisted for about five months and then disappeared. In June 2002, fifteen years postoperatively, the tooth had a normal sulcus and was asymptomatic (see figures 9[22] and 10[23]).
Case#4
In June 1990, a female patient presented with tooth #3 fractured through the furcation. This tooth also had existing endodontic treatment and amalgam restoration. It was clamped, and filled with GlasIonomer® Base Cement (Shofu) prepared for a porcelain fused to metal crown, which was placed three weeks later. As of June, 2002, the tooth was normal and asymptomatic (see figures 11[24] and 12[25]).
The author has treated a number of other cases besides the ones mentioned above, with lesser degrees of photographic documentation. In those cases where the fracture has not been treated within a couple of days, or where the tooth was not protected sufficiently from re-injury, a periodontal defect developed with attendant abscess formation and case failure. Where attention to the injury was prompt and stabilization absolutely secure, success has been the result.
Description of repair technique:
- Diagnosis: The fracture, of course, is confirmed by verifying the independent mobility of sections of the tooth. If the two sections of the tooth are each only slightly mobile, the fracture is through the furcation or runs deep, apically. These fractures are actually easier to treat. However, the fracture can be quite shallow, involving a cusp that has sheared off to a fracture line only several millimeters below the attachment.
- Cleansing: The object is to remove all debris from inside the fracture. I prefer to clean the wound with a 30% hydrogen peroxide solution (Superoxol®, Sultan) and then rinse with water.
- Reduction: This step is critical. You need to get the fractured segments back into perfect apposition. A rubber dam clamp is an excellent way to hold the pieces together as you go through the next steps. Deeper fractures are easier to stabilize at this step. A fracture that is just below the attachment may be very difficult to clamp securely, because the fracture line is fairly oblique.
- Bonding: Do not attempt to get bonding agent between the faces of the fracture. This only introduces a chance for error and failure by creating a microscopic space between the fractured segments. Additionally, it is impossible to prevent contamination of the bond from tissue fluid as you clamp the pieces together. Instead, after reducing the fractured segments and holding them with a rubber dam clamp, cut a groove along the fracture, and place your bonding agent and composite into that groove. Cut the groove deep enough to allow plenty of bonding surface but not so deep that you risk perforation or destabilization of the clamp. If you prefer an amalgam technique, you can also cut a butterfly prep into each segment and condense amalgam into the prep and leave the clamp on the tooth for an hour.
- Preparation and temporization: After the bonding is secure, proceed immediately to crown preparation. Do not allow the tooth to function while being held only by the bonding, as the risk of re-fracture is too great. Prepare the tooth for a crown, take your impression, and place a temporary crown. If possible, you may want to keep the clamp on the tooth during most or all of the preparation. Either a stainless steel crown or an aluminum shell crown lined with acrylic can serve as a temporary. In the case of the latter, I recommend allowing the acrylic to harden in the shell while on the tooth and then not touching it. The fractured segments must be kept absolutely immobile with respect to each other in order for healing to be successful.
- Endodontic treatment, if necessary: If the fracture is through the pulp, endodontic treatment will likely be necessary. However, treatment is not possible until the segments are stabilized. Therefore, you should stabilize the segments first with bonding, and then address the endodontic situation. The rubber dam clamp placed on the tooth during endodontic treatment will help insure that the segments are not inadvertently separated during the course of treatment. I prefer doing the crown preparation first, and then doing the endodontic treatment through the temporary crown.
- Placement of the crown: The crown should be extremely strong – either porcelain fused to metal or full cast metal is recommended. Place it as soon as possible, because the longer the temporary crown is on, the greater the risk that the temporary may fall off or break and ruin the case.
Conclusions:
This paper has examined literature which establishes that cementum deposition in humans continues beyond the period of tooth formation and thus establishes that cementum repair of fractured teeth is theoretically possible.
Additionally, four cases have been presented with histories of from nine to twenty-one years. Each case involved a tooth fracture that extended from supragingival to subgingival areas. In each case, the tooth continues to function for the patient with no periodontal pathology.
I present as a hypothesis, the following principles of successfully restoring a root fracture:
- The fracture must be treated immediately – within a couple of days.
- The reduction of the fractured pieces must be complete and perfect.
- From the first day, the repair must be made absolutely stable.
- If the above conditions are met, a fracture that extends below the gingival attachment will eventually heal and will have an excellent long-term prognosis. I hypothesize that the periodontal ligament cells deposit new cementum over the fracture and thus, with proper healing, there is no potential for infection from the fracture site.
There are several possible explanations for the need for immediate reduction of the fracture. One may be that the fracture line can become a nidus of infection. If enough time elapses before the pieces are reduced, there is a possibility of tissue swelling or other debris getting into the fracture site and not being able to be removed completely, thus preventing perfect apposition of the fragments. The space created then may provide a constant source of infection and irritation that prevents complete healing. If, on the other hand, the pieces can be brought into perfect re-alignment, the irritants are minimized and the periodontal ligament can deposit new cementum over the fracture, thus providing optimal healing.
Another factor at work may be the health of the periodontal ligament fibers that are in the immediate proximity of the fracture. If, due to the movement of the fractured segments, they continue to be traumatized, healing potential could be compromised.
Footnotes and images
[1] Walton, R.E. Principles of endodontics, ed. 2. Philadelphia, W.B.Saunders Co., p 485. 1996.
[2] Stanley, J.R. The cracked tooth syndrome. J Am Acad Gold Foil Operators 11:36-47, 1968.
[3] Snyder, D.E. The cracked-tooth syndrome and fractured posterior cusp. Oral Surg 41:698-704, 1976.
[4] Ritchie, B..; Mendenhall, R.; and Orban, B. Pulpitis resulting from incomplete tooth fracture. Oral Surg, Oral Med, Oral Pathol 10:665-671, 1957.
[5] Linaburg, R.G. and Marshall, F.J. The diagnosis and treatment of vertical root fractures: report of case. JADA 86:679-683, 1973.
[6] Plant, J.J., and Uchin, R.A., Endodontic failures due to vertical root fractures: two case reports. J Endodont 2:53-55, Feb. 1976.
[7] Simon, J.H.S.; Glick, D.H.; and Frank, A.L. Predictable endodontic and periodontic failures as a result of radicular anomalies. Oral Surg 31:823-826. June 1971.
[8] Lefkowitz, W. The formation of cementum. Am J Ortho 30:224-240. May 1944.
[9] Hammer, H. Die Heilungsvorgänge bie Wurzelbrüchen. Deutsch Zahn Mund Kieferheilk 6:297, 1939.
[10] Andreasen, J.O., and Hjørting-Hansen, E. Intraalveolar root fractures: radiographic and histologic study of 50 cases. J Oral Surg 25:414-426. Sept. 1967.
[11] Hall, D.A. Restoration of a shattered tooth – report of a case. JADA 129:105, Jan. 1998.
[12] Masaka N. Long-term observation of fractured tooth roots preserved by adhesion. Adhesive Dentistry. Japanese 13:156-170, 1995.
[13] Aouate, G. Treatment of an intra-alveolar root fracture by extra-oral bonding with adhesive resin. Information Dentaire. French 26:2001-2008, 2001.

Case #1—Tooth #3 does not appear fractured.
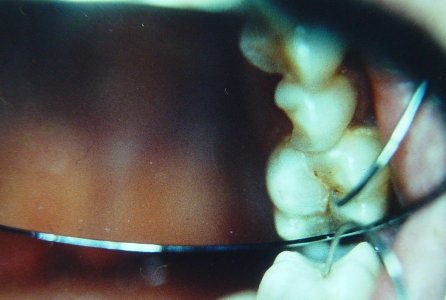
Case #1—explorer used to separate fragments, confirming fracture.

Case #1—tooth partially prepared for crown, showing fracture line.

Case #1—tooth with fracture bonded, prepared for crown, and ready for impression.

Case #1—10-year post-operative view.
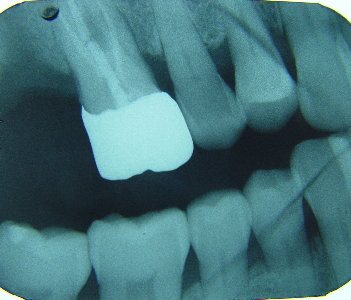
Case #1—10-year post-operative radiograph.

Case #2—14-year post-operative view.

Case #2—21-year post-operative radiograph.
Case #3—15-year post-operative view.

Case #3—15-year post-operative radiograph.

Case #4—12-year post-operative view.
Case #4—12-year post-operative radiograph.
If you have a broken front tooth, broken completely above the gumline, an expert cosmetic dentist can fix that with direct bonding in a single appointment, and it will look beautiful.
See Dr. Hall’s blog posts where he has fielded questions about fractured teeth.