Dr. Hall,
I had a tooth extraction, but the root was left there because apparently there’s bone in-between and the dentist would have to do bone reduction to remove the root. She said we wait and see. Do I need to worry about it? I have been given antibiotics.
– Kavya from Broadview, South Australia
(See Dr. Hall’s answer below.)
We thank our advertisers who help fund this site.
Kavya,
I have written about this category of situation before. During a particularly difficult extraction, sometimes a root tip of the tooth can break off and it can be prudent to leave the root tip in to avoid the complications of going after it. Azila from Kuala Lumpur asked me a question about leaving a root tip in the jawbone several years ago. I told her that in her case, yes, it could be too risky to go after the root tip.
The decision about leaving a part of the root in the bone should be based on two issues. The first is, How big is the piece? The smaller the piece, the smaller the risk. There is pulp tissue inside a root, and the more of that there is, the greater the chance of a problematic infection.
The second issue is, What is the risk of going after the root tip? For lower teeth, especially molars, the root tips can be very close to the inferior alveolar nerve. Damage to that nerve could cause permanent numbness to the lower teeth on that side of the jaw and to the lower lip on that side. With upper molars, the roots can be very near the maxillary sinus and trying to get a root tip out could cause it to be pushed into the sinus, requiring sinus surgery to remove it.
It doesn’t sound to me like your case fits in this category. You said that “the root” was left in the bone, which sounds like the entire root. That isn’t a small root tip. Second, the reason your dentist seems to have given is that “bone reduction” would have to be done to remove the root. That sounds like extra work, and not some health risk to you. And removing some bone is often required for an extraction&mash;that shouldn’t be a big deal. If I am accurately understanding what happened here, your dentist should have admitted that she didn’t have the needed skills to remove the bone to finish this difficult extraction and should have referred you to an oral surgeon to complete it. The fact that she gave you antibiotics suggests to me that she understands that there is a risk of infection from the piece that was left in. This infection would arise from the pulp tissue that is in the tooth root that was left. The problem here is that the antibiotics will tamp down the infection but won’t eliminate it and, when you are done taking the antibiotics, there is an excellent chance that the infection could flare up again and this time be antibiotic-resistant.
I would find an oral surgeon and go there for a second opinion. And I would do it before the hole left by your missing tooth heals over. Finishing the extraction will be much easier if it hasn’t fully healed.
I hope this is helpful.
– Dr. Hall
Do you have a comment or anything else to add? We’d love to hear from you. Enter your comment below. Or click here to ask Dr. Hall a question.
About David A. Hall
Dr. David A. Hall was one of the first 40 accredited cosmetic dentists in the world. He practiced cosmetic dentistry in Iowa, and in 1990 earned his accreditation with the American Academy of Cosmetic Dentistry. He is now president of Infinity Dental Web, a company in Mesa, Arizona that does advanced internet marketing for dentists.


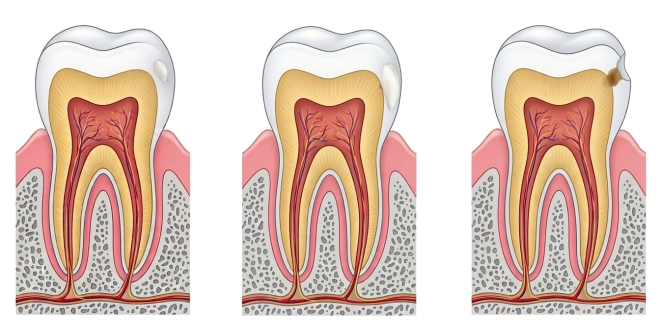
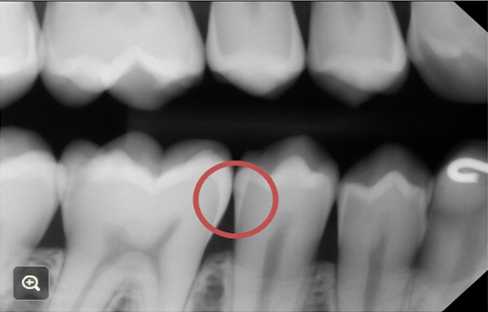 For a more accurate picture of the decay process, I found this x-ray. Look at the area that is circled. The molar on the left has a very superficial caries lesion that is still in the enamel. The premolar on the right has a v-shaped caries lesion that has barely penetrated the enamel and there is a very slight darkening in the dentin.
For a more accurate picture of the decay process, I found this x-ray. Look at the area that is circled. The molar on the left has a very superficial caries lesion that is still in the enamel. The premolar on the right has a v-shaped caries lesion that has barely penetrated the enamel and there is a very slight darkening in the dentin. So what is a natural smile? Exploring this idea, I asked ChatGPT to create an image of a woman with a natural smile, and on the right is what it came up with. That’s pretty close to my idea of a natural smile.
So what is a natural smile? Exploring this idea, I asked ChatGPT to create an image of a woman with a natural smile, and on the right is what it came up with. That’s pretty close to my idea of a natural smile.