Dr. Hall,
I had my upper 6 front teeth pulled due to periodontal disease. I was going to have 4 implants with two pontics, but asked for something less expensive. So we are talking about doing a permanent bridge. I have read about the Maryland Bridge and feel now that maybe the separate implants with two pontics would be better? They have charged me the same price so my question is …would 4 implants and two pontics be better?
– Jill from Pennsylvania
(Note from Dr. Hall – a pontic is the false tooth part of a dental bridge.)
Jill,
I can’t really prescribe anything specific for your case without seeing you, but I can be some help here by giving you some guidance from basic principles of bridges and restorative dentistry.
If you are accurately telling me what your dentist is telling you, then something is very wrong here. A permanent dental bridge replacing six missing upper front teeth on any patient with significant gum disease would be a disaster waiting to happen. It’s not going to last, and in the end will be by far the most expensive option. Other options would be far better in multiple ways. And I’ll explain why. I’m going to explain this in some detail here for you and then use this explanation as a blog post that will hopefully help others with similar questions.
Here is a diagram of your upper arch:
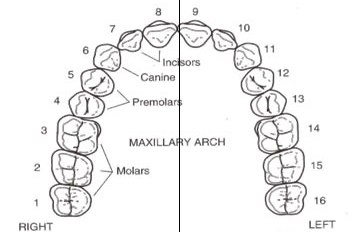
So you are saying that you have had the front teeth extracted, which would be teeth numbers 6 through 11.
Here are a couple of principles of doing bridgework that every dentist is taught in dental school.
First, any bridge needs to be supported by teeth that collectively have the same amount of support as the missing teeth. In other words, if the bridge is replacing two medium-sized teeth, it needs to be anchored by at least two medium-sized teeth. If four small teeth are missing, they could maybe be supported by two large teeth, if those supporting teeth are twice as large as the missing teeth. So, you are missing four medium-sized teeth (6, 8, 9, and 11) and two small teeth (7 and 10). To support that adequately, you need four medium-sized teeth (4, 5, 12, and 13) and probably one large tooth (3 or 14). So you are ending up with an extremely complicated 11-unit bridge, consisting of six false teeth supported by five existing teeth. Now I suspect that your dentist, especially if you are pressing to save money, may be planning something less than this. But breaking this rule would severely limit the lifespan of the bridge.
Second, when you start adding supporting teeth, you increase the likelihood of failure for two reasons. One is that each supporting tooth has to be prepared to be perfectly parallel to all the other teeth. Getting five prepared teeth to be all parallel to each other (or even four) so that the bridge fits perfectly is extremely demanding, and I would not ask a regular family dentist to do that. When you add to that complication the problem of having teeth on opposite sides of your mouth, making those parallel is a very tricky proposition. Another reason is that if you have any kind of trouble down the road with any of the supporting teeth – decay or gum disease or any other significant problem – the entire bridge will have to be re-done. How expensive is that going to be? Way more than implants.
Third, with six missing front teeth you have what is called a cantilever effect. Look at the diagram and imagine that tooth #4 is missing. This tooth could be replaced with a simple three-unit bridge – the missing tooth #4 supported by teeth #s 3 and 5. Notice that these teeth are pretty much in a straight line. There would be no tipping forces at all when chewing stress is borne by tooth #4. This is the type of stress these supporting teeth are designed to take. But now compare this with teeth #s 6 through 11. These are on a curve. The strongest bridge between teeth #s 5 and 12 would be on a straight line between the two teeth. But that kind of a bridge would go across the roof of your mouth and wouldn’t make any sense. So we have to loop the bridge out around the curve. Have you ever seen a highway bridge that curves out like that? Of course not. They always form a straight line between the supports. The reason for that is that when you’re out on that curve, you create tipping forces which put a large amount of stress on not only the supporting structures but the entire bridge. This force becomes a force that wants to twist and push the two closest anchors (#s 5 and 12) and actually pull the remaining anchors out of their sockets. These are stresses that these teeth are not designed to take, and the life expectancy of such a bridge would be pretty short. You would probably end up losing all of the anchor teeth, in addition to the six you are already missing. To compensate for that added stress factor, your dentist could try anchoring with six teeth instead of five. But then you increase the risk also and may end up losing all six of them.
The conclusion of all this is that a permanent bridge replacing six front teeth would be a bad idea for someone with healthy gums in the hands of some of the most expert dentists in the country. When you add the complicating factor that you have significant gum disease, and add that to the possibility that your dentist may be an average family dentist, you are courting disaster.
So what should you do?
Anything other than the fixed bridge. Don’t end up in our collection of cosmetic dentistry horror stories.
The most economical solution would be a removable partial denture. With today’s acrylics, this could be made to be very esthetic and could have clear acrylic clasps that would be virtually invisible to anyone else. There are some inconveniences to having a removable partial denture, but the cost would be a small fraction of the cost of any other option.
The most comfortable and highest quality solution would be using dental implants. Now whether or not you could support the false teeth with two or four implants would depend on how much bone support you have and the stress of your bite.
My advice? Get a second opinion from an excellent dentist. (See my posts about how to ask for a second opinion.) There is an excellent dentist near you with a national reputation. I’ll send you his name as well as another who is quite a bit further for you but whose fees would be considerably lower. Some dentists will give second opinions for free. But even if you pay $100 for it, that would be much more sensible rather than throwing $10,000 or more at a solution that may only last a few months, even if you don’t end up having the second dentist do the work.
Dr. Hall
|
We thank our advertisers who help fund this site.
|
|
About David A. Hall
Dr. David A. Hall was one of the first 40 accredited cosmetic dentists in the world. He practiced cosmetic dentistry in Iowa, and in 1990 earned his accreditation with the American Academy of Cosmetic Dentistry. He is now president of Infinity Dental Web, a company in Mesa, Arizona that does advanced internet marketing for dentists.
 It sounds like you have an overhang, and, if I am understanding you correctly, I disagree strongly with your dentist. An overhang is a margin irregularity that comes from the dentist having problems with the impression that was taken after your tooth was prepared for the veneer. The impression didn’t accurately record the end of the preparation making it so the laboratory technician couldn’t create the veneer to leave a smooth finish line between the veneer and the tooth.
It sounds like you have an overhang, and, if I am understanding you correctly, I disagree strongly with your dentist. An overhang is a margin irregularity that comes from the dentist having problems with the impression that was taken after your tooth was prepared for the veneer. The impression didn’t accurately record the end of the preparation making it so the laboratory technician couldn’t create the veneer to leave a smooth finish line between the veneer and the tooth.  The end result needs to be that the veneer replicates the original contour of the tooth at the gumline, as shown in the top drawing on the right. The bottom drawing shows a slight overhang—there isn’t a perfectly smooth transition from the veneer to the tooth. If that occurred with a veneer I had placed, I would replace it for no charge.
The end result needs to be that the veneer replicates the original contour of the tooth at the gumline, as shown in the top drawing on the right. The bottom drawing shows a slight overhang—there isn’t a perfectly smooth transition from the veneer to the tooth. If that occurred with a veneer I had placed, I would replace it for no charge. Here’s a drawing showing a normal contour of the crown on the left, and overcontouring of the crown on the right. The drawing doesn’t show a normal gumline—usually the margin of the crown will be under the gumline. Overcontouring of the crown causes two problems. First, it puts pressure on the gum. Second, it creates a trap for food particles under the bulge of the crown. Both of these contribute to irritation of the gums, causing gum disease which results in redness, swelling, and bleeding of the gums.
Here’s a drawing showing a normal contour of the crown on the left, and overcontouring of the crown on the right. The drawing doesn’t show a normal gumline—usually the margin of the crown will be under the gumline. Overcontouring of the crown causes two problems. First, it puts pressure on the gum. Second, it creates a trap for food particles under the bulge of the crown. Both of these contribute to irritation of the gums, causing gum disease which results in redness, swelling, and bleeding of the gums.

 what happens when crowns are too thick. It creates a protected space where the crown meets the tooth and in that protected space, gum-disease-causing bacteria multiply freely. Microscopic food particles will get trapped there, it is impossible to clean effectively, with resulting
what happens when crowns are too thick. It creates a protected space where the crown meets the tooth and in that protected space, gum-disease-causing bacteria multiply freely. Microscopic food particles will get trapped there, it is impossible to clean effectively, with resulting